Can Throat Exercises Really Reduce Snoring and Sleep Apnoea?
Most people, when they discover they have a snoring problem or are diagnosed with obstructive sleep apnoea, find themselves confronted with a fairly unappetising menu of options. There is the CPAP machine — effective, evidence-based, and tolerated by roughly half the people who try it long-term. There are mandibular advancement devices, which move the jaw forward during sleep and work well in the right patients. There is sleep apnoea surgery London, which I perform regularly and which produces excellent results when the anatomy is right. And then, sitting quietly at the end of the table and rarely getting a proper introduction, there are throat exercises.
I want to give them a proper introduction here. Because the evidence behind them is considerably stronger than most patients — and, frankly, many clinicians — realise.
What are throat exercises, and why do they work?
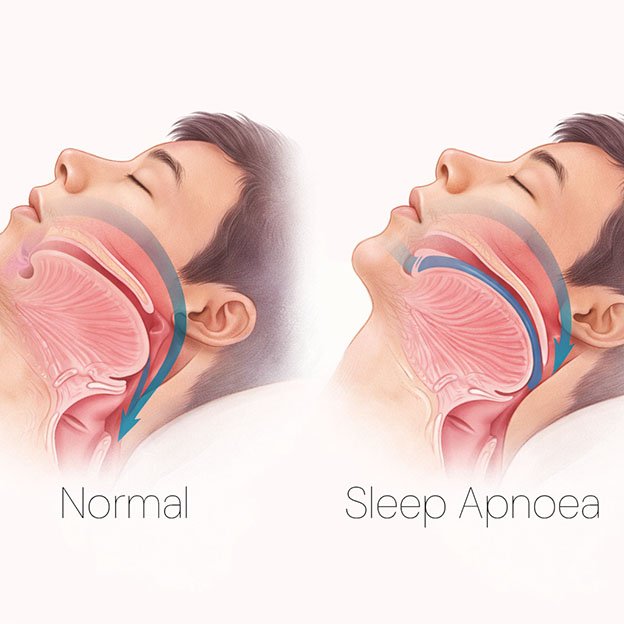
The approach goes by several names: myofunctional therapy, oropharyngeal exercises, or simply throat and tongue exercises. The principle is straightforward. The upper airway is lined with muscle. During sleep, that muscle relaxes. If it lacks sufficient tone, the airway narrows, soft tissue vibrates, and you snore. In more severe cases, the airway collapses partially or fully, breathing stops momentarily, the brain rouses you just enough to restore airflow, and the cycle repeats — sometimes hundreds of times a night. That is obstructive sleep apnoea.
The question the research has been trying to answer for the past decade is whether structured exercise can improve the baseline tone of these muscles sufficiently to make a clinical difference. The answer, as of 2025, is a fairly confident yes — with some important caveats I will come to.
What does the research actually show?
The foundational paper in this field is Camacho and colleagues' 2015 systematic review and meta-analysis, published in the journal Sleep. They pooled data from multiple studies and found that oropharyngeal exercises reduced AHI — the apnoea-hypopnoea index, which measures breathing interruptions per hour of sleep — by approximately 50% on average. They also found improvements in minimum overnight oxygen saturation and in daytime sleepiness scores. This was not a small effect. A 50% reduction in AHI can move a patient from moderate sleep apnoea to mild, or from mild to below the diagnostic threshold entirely.
That finding has been replicated and extended by subsequent research. Saba and colleagues published a systematic review and meta-analysis in The Laryngoscope in 2023 confirming clinically relevant reductions in AHI alongside improvements in snoring and daytime sleepiness. A 2025 network meta-analysis by Xu and colleagues confirmed AHI reductions of approximately nine to ten events per hour compared to controls, along with improved minimum SpO2 and Epworth Sleepiness Scale scores. Pisoni and colleagues published an overview and re-analysis of existing systematic reviews in the Journal of Sleep Research in 2025, again confirming the findings hold across multiple independent research groups.
The credibility anchor for sceptics is the Cochrane Collaboration review by Rueda and colleagues, published in 2019. The Cochrane Database of Systematic Reviews is the highest tier of evidence synthesis in medicine. It demands pre-registered methodology, independent checking, and formal risk-of-bias assessment. Rueda et al. concluded that oropharyngeal exercises reduce OSA severity, snoring frequency and intensity, and daytime sleepiness in adults compared with control conditions. This is not fringe research or wellness industry wishful thinking. It is mainstream peer-reviewed evidence.
For snoring specifically — relevant to the large number of people who snore disruptively but do not have clinically significant sleep apnoea — the data are similarly encouraging. A separate 2018 systematic review by Camacho and colleagues found a 31% reduction in the proportion of the night spent snoring, along with a 36 to 51% reduction in subjective snoring intensity. A 2025 randomised controlled trial by Alheija and colleagues added further RCT-level evidence confirming the snoring benefit specifically.
"The advice provided by Vik Veer has resulted in an immediate fixing of my sleep apnoea. My AHI was 24 prior to using CPAP 18 months and 15 after using. After using the techniques he recommended, it has fallen to 1! It is unusual to find someone who understands sleep apnoea and provides practical techniques to eliminate symptoms." Google Review, 5 stars — Peter Hurley
Exercises with evidence behind them
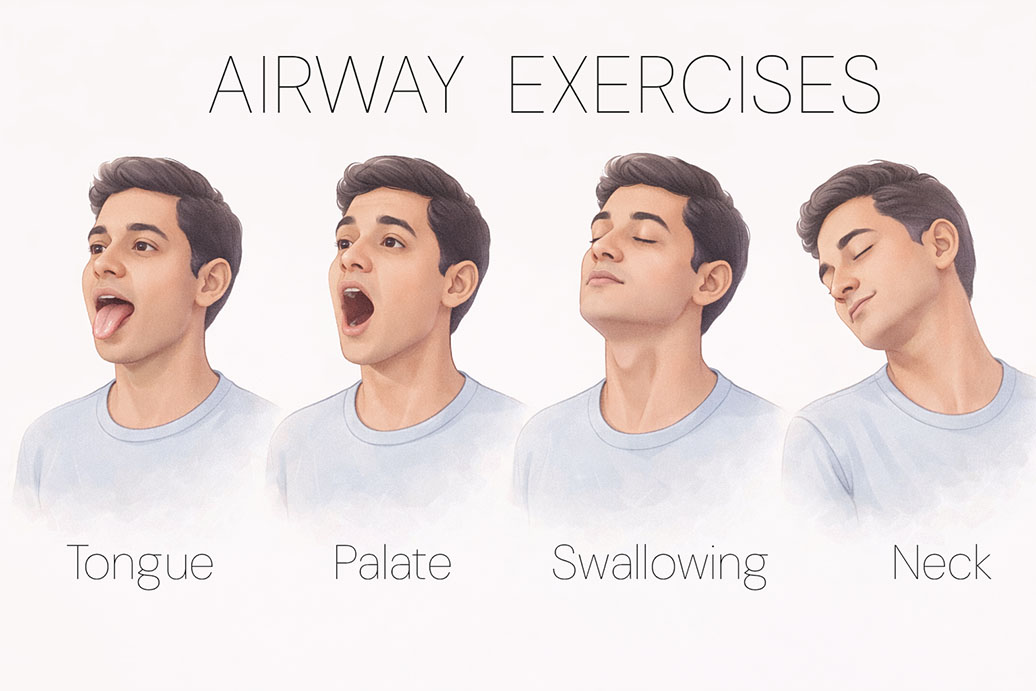
Not every exercise that gets labelled a "throat exercise" is mechanistically sound. The following are the targets with the strongest evidence: tongue, palate, throat, and breathing.
| Exercise | What it does | Evidence base |
|---|---|---|
| Tongue press — press tongue firmly to roof of mouth and hold | Tones the genioglossus, the main muscle preventing tongue collapse into airway | Referenced across multiple meta-analyses including Camacho 2015, Saba 2023 |
| Tongue slide — slide tip of tongue backwards along palate as far as possible | Activates posterior tongue and soft palate simultaneously | Camacho 2015, De Felicio 2018 |
| Soft palate elevation — sustained vowel sounds ("aaah"), singing | Directly tones the uvula and soft palate — the structures most associated with snoring vibration | Koka 2021 (pathophysiological mechanism), Camacho 2018 snoring meta-analysis |
| Swallowing retraining — correct tongue posture during swallow, repeated sets | Recruits full pharyngeal musculature; retrains resting tongue position | De Felicio 2018, Saba 2023 |
| Nasal breathing training — deliberate nasal-only breathing during exercise and rest | Restores nasal airflow, reduces mouth breathing and associated pharyngeal collapse | Carrasco-Llatas 2021, Xu 2025 network meta-analysis |
| Throat/pharyngeal resistance exercises — gargling with sustained tone, or resisted swallowing | Targets lateral pharyngeal walls — a key collapse point in OSA | Koka 2021 pathophysiology paper, Rueda 2019 Cochrane review |
Why the right approach matters: understanding the mechanism
The airway is not simply a passive tube. It is a dynamic structure held open by the coordinated action of numerous muscle groups: the genioglossus, which pulls the tongue forward; the muscles of the soft palate and uvula; the lateral pharyngeal wall muscles; and others. During wakefulness, these muscles maintain sufficient tone to keep the airway patent. During sleep, particularly in the deeper stages, that tone diminishes. If the baseline resting tone is low — due to age, weight gain, or simple disuse — the reduction during sleep tips the airway into collapse.
The goal of oropharyngeal exercise is to raise that baseline resting tone. Not to build bulk — this is a critical distinction, and one I emphasise to patients. Hypertrophied pharyngeal tissue can actually narrow the airway lumen, which is the opposite of what we want. The target is functional tone: enough stiffness and neuromuscular coordination to resist collapse during sleep. Think of it as physiotherapy for a functional deficit, not training for athletic performance.
Who responds best? Clinical observations
From my own clinical experience, I would add a few observations that do not yet appear prominently in the published literature but that I find influence outcomes considerably. First, patients who developed snoring in middle age — who were quiet sleepers in their 30s and gradually became snorers through their 40s and 50s — tend to respond considerably better than lifelong snorers. If snoring has been present since early adulthood, a structural cause is more likely — a narrow jaw, adenotonsillar hypertrophy, a significantly deviated septum — and exercise alone is unlikely to be curative.
Second, patients with enlarged tonsils or significantly blocked nasal passages get limited benefit from exercises alone. The exercises work on the muscular component of airway obstruction. They cannot address anatomical bulk or fixed structural narrowing. For these patients, I would suggest addressing the structural issue first, after which exercises may well have a role. Third, and most importantly: adherence is everything. The trials showing 50% AHI reduction used daily practice of at least 30 minutes. A casual five-minute routine before bed will not produce the effect sizes in the published literature.
The daytime consequences — and why they matter
The daytime consequences of sleep-disordered breathing are worth dwelling on, because they are often more immediately motivating for patients than the abstract long-term health risks. Fragmented sleep — even when the individual arousals are too brief to remember — produces non-restorative sleep. Patients wake feeling exhausted despite adequate time in bed. The standard clinical measure is the Epworth Sleepiness Scale, which runs from zero to 24 with scores above ten indicating abnormal daytime sleepiness. Multiple meta-analyses now show oropharyngeal exercises improving ESS scores by three to six points — which is often the difference between scoring in the abnormal range and scoring normal. Beyond quality of life, excessive daytime sleepiness has implications for driving safety and occupational performance.
The oxygen findings deserve equal attention. Overnight oxygen desaturation — the repeated drops in blood oxygen that accompany each apnoea — is the primary driver of the long-term cardiovascular consequences of untreated sleep apnoea: hypertension, atrial fibrillation, coronary artery disease, increased stroke risk. Multiple RCT-only meta-analyses now demonstrate that oropharyngeal exercises improve minimum nocturnal SpO2 in adults with OSA. The effect size is not as large as CPAP in severe disease, and I want to be direct about that. But in patients with mild to moderate OSA, in patients who cannot tolerate CPAP, or in patients using exercises as an adjunct to other treatments, an improvement in minimum oxygen saturation has genuine cardiovascular relevance.
The Best Evidence
The Cochrane Collaboration — the gold standard for evidence review — published a review of these exercises in 2019 (Rueda et al.), and a 2025 overview in the Journal of Sleep Research confirmed the findings hold up across multiple systematic reviews.
Benefits are strongest with daily practice of at least 30 minutes and good adherence. When patients tell me exercises did not work for them, the first question I ask is how consistently and how long they actually practised. The answer is usually revealing.
Being honest about limitations

Most trials are short — weeks to months rather than years — so long-term durability of benefit is not well established. The optimal combination and sequencing of exercises has not been definitively determined; protocols vary considerably across studies. Evidence in children is sparse, and most paediatric OSA has a structural aetiology that exercise is unlikely to substantially address. For moderate to severe OSA, exercises function as an adjunct to established treatments rather than a replacement. I would not advise a patient with an AHI of 45 to cancel their CPAP appointment and start gargling instead.
But for the large population of people with primary snoring, mild OSA, or moderate OSA who are CPAP-intolerant, the case for oropharyngeal exercises as a meaningful first-line or complementary intervention is now well-supported by the evidence. For anyone exploring sleep apnoea treatment without CPAP, exercises deserve to be near the top of that list. There are no side effects. There is no cost. The exercises can be done at home without equipment or supervision.
"Mr Veer is kind, personable and very knowledgeable. I had an initial online consultation with him to discuss treatment for my sleep apnoea. I now feel well informed and hopeful about the treatment of my long-standing sleep problems." Google Review, 5 stars — Adam Rutherford
Why you probably haven't heard this from your doctor
The reason exercises often do not come up is, I suspect, structural rather than evidential. There is no product to sell. No device company funds awareness campaigns for tongue presses. No pharmaceutical sponsor runs patient information initiatives for gargling exercises. The knowledge sits in journals, gets cited in meta-analyses, and is confirmed by Cochrane reviews — and then largely fails to reach the people it could help. As a snoring surgeon London, I believe it is part of my role to change that.
If you want the full exercise protocol — which exercises, in what order, how long, and what realistic expectations look like — you will find it in my newsletter. And if you have questions about whether your particular pattern of snoring or sleep apnoea is likely to respond, I am happy to help you think through that too.
What are you doing about it?
I am currently developing a structured airway muscle training programme designed to help people improve snoring, sleep apnoea and breathing stability by training the muscles of the tongue, palate, throat and breathing system. The programme is based on the same principles used in rehabilitation medicine: activation first, then endurance and control. I will be releasing it soon.
If you would like to be among the first to learn about it, join my newsletter here.
Subscribe NowReferences
Alheija, A. et al. (2025). Effects of orolingual myofunctional therapy on snoring: a randomised controlled trial. Acta Oto-Laryngologica, 145, 857–865.
Camacho, M. et al. (2015). Myofunctional therapy to treat obstructive sleep apnoea: a systematic review and meta-analysis. Sleep, 38(5), 669–675.
Camacho, M. et al. (2018). Oropharyngeal and tongue exercises (myofunctional therapy) for snoring: a systematic review and meta-analysis. European Archives of Oto-Rhino-Laryngology, 275, 849–855.
Carrasco-Llatas, M., O'Connor-Reina, C. and Calvo-Henríquez, C. (2021). The role of myofunctional therapy in treating sleep-disordered breathing. International Journal of Environmental Research and Public Health, 18, 7291.
De Felicio, C., Dias, F. and Trawitzki, L. (2018). Obstructive sleep apnoea: focus on myofunctional therapy. Nature and Science of Sleep, 10, 271–286.
Koka, V. et al. (2021). Orofacial myofunctional therapy in obstructive sleep apnoea syndrome: a pathophysiological perspective. Medicina, 57, 323.
Pisoni, E. et al. (2025). Myofunctional therapy in adults and children with obstructive sleep apnoea: an overview and re-analysis of systematic reviews. Journal of Sleep Research, e70219.
Rueda, J. et al. (2019). Myofunctional therapy (oropharyngeal exercises) for obstructive sleep apnoea. Cochrane Database of Systematic Reviews, 11, CD013449.
Saba, E. et al. (2023). Orofacial myofunctional therapy for obstructive sleep apnoea: a systematic review and meta-analysis. The Laryngoscope, 134.
Xu, Y. et al. (2025). Efficacy of myofunctional therapy for obstructive sleep apnoea: a systematic review and network meta-analysis. Journal of Evidence-Based Dental Practice, 25(3), 102137.
Zhang, F. et al. (2022). The efficiency of orofacial myofunctional therapy in treating obstructive sleep apnoea: a meta-analysis of observational studies. Journal of Oral Rehabilitation.
Contact Professor Vik Veer
If you would like to know more or to arrange a consultation, please use the links below.
If you would like more information please contact Prof Vik Veer via his team of secretaries:
Private secretary: 0207 458 4584
Email: Secretary@Consultant-Surgeon.co.uk